| Prashant Kedia, MD from the Division of Gastroenterology and Hepatology, Weill Cornell Medical College at Cornell University in New York, New York, USA shares this video case “Hemorrhagic pancreatic necrosis drainage by using an esophageal stent.” |
|

| This video highlights the case of a patient with infected hemorrhagic pancreatic necrosis treated with endoscopic debridement through a fully covered metal esophageal stent. Initially, double pigtail plastic stents were placed due to the fluid nature of the contents. However due to an acute bleeding event into the collection possibly secondary to a pseudoaneurysm, the patient developed hemorrhagic pancreatic necrosis which subsequently became infected. To endoscopically manage this situation, direct necrosectomy was required via EUS-guided placement of a fully covered metal esophageal stent with through-the-scope deployment into the walled-off hemorrhagic pancreatic necrosis. Through this multiple techniques for debridement including usage of snares and nasocystic drains were applied to evacuate the cavity. |
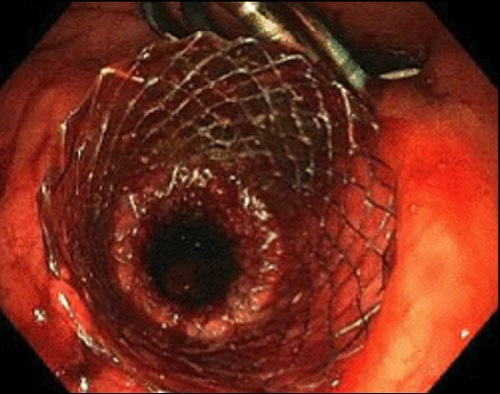 |
| This video is useful to portray the advantage of using fully covered metal stents for walled off pancreatic necrosis compared to plastic stents. Due to large lumenal diameter of these metal stents, they allow for direct endoscopic necrosectomy and removal of large solid material. Although only one metal stent is currently approved for pseudocyst drainage in the United States, fully covered, through-the-scope esophageal stents can also be used in these situations. The application of EUS-guided cystgastrostomies with fully covered metal esophageal stents have been shown in prospective case series to allow for successful endoscopic necrosectomy of walled off pancreatic necrosis. These stents allow for maintenance of a gastrocystic fistula through which multiple necrosectomy sessions can be performed and a nasocystic drain can be placed for continuous flushing. Find more VideoGIEs available online. The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth. |
|