| Shuntaro Mukai from the Department of Gastroenterology and Hepatology at Tokyo Medical University in Tokyo, Japan describes this VideoGIE case “Pulsating pseudoaneurysm in a walled-off necrosis.” |
|

| Our video case describes a pulsating pseudoaneurysm in the cavity of a walled-off necrosis (WON) diagnosed by endoscopy through a fully-covered biflanged metal stent (BFMS). Subsequently, the pseudoaneurysm was successfully treated. A 38-year-old man developed an infected WON after severe necrotizing pancreatitis. A novel BFMS (16 mm in diameter and 20 mm in length) was placed under EUS guidance. Then, direct endoscopic necrosectomy (DEN) was performed through the BFMS. Seven days after DEN, he vomited blood; we suspected bleeding from the cavity. Emergency angiography was not able to detect any obvious bleeding point. After seven days of conservative therapy, an endoscope was advanced to examine the condition within the cavity. Surprisingly, a pulsating pseudoaneurysm was found. Subsequently, the pseudoaneurysm was treated by coil embolization. Interestingly, a “second-look” endoscopy determined that the pseudoaneurysm completely resolved after use of the embolization coil. To the best of our knowledge, this is the first video which shows a pulsating pseudoaneurysm detected by direct endoscopic imaging and subsequently successfully treated by coil embolization. Bleeding from the cavity due to the rupture of a pseudoaneurysm is a fatal complication in patients with WON. Thus, the management of bleeding is mandatory for treatment success. BFMS is useful for the treatment of WON also in that observation in the cavity of WON by endoscopy can be easily performed during the treatment course. Find more VideoGIEs available online. |
|
|
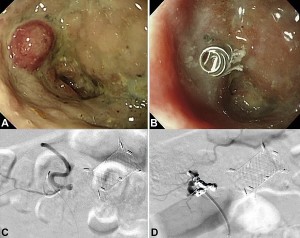
Figure 1. Endoscopic imaging revealed a pulsating pseudoaneurysm (A). A “second-look” endoscopy demonstrated that the pseudoaneurysm completely resolved after use of the embolization coil (B). Angiography revealed a pseudoaneurysm (C), which was subsequently treated by coil embolization (D). |
| The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth. | |