| Ryosuke Tonozuka, MD, from the Depatment of Gastroenterology and Hepatology at Tokyo Medical University in Tokyo, Japan discusses this New Methods article “EUS-guided drainage of hepatic abscess and infected biloma using short and long metal stents (with videos).” |
|

| Refractory hepatic abscess (HA) and infected biloma (IBL), in which inflammation does not improve only by the dosage of the antibiotic agent, often require percutaneous drainage (PCD) and surgical interventions. Recently, the usefulness of EUS-guided hepatic abscess drainage (EUS-HAD) and US-guided biloma drainage (EUS-BLD) has been described. However, there has been only 1 report of a case in which a fully covered self-expandable metal stent (FCSEMS) was used. In this study, we evaluated the safety and efficacy of EUS-HAD and EUS-BLD using a FCSEMS retrospectively. We used 2 types of FCSEMSs for the drainage. If the target lesion was close to the digestive tract (≤2 cm), a short biflanged FCSEMS (short stent; 16 mm in diameter, 2 or 3 cm in length) was used. If the target lesion was far (≥3 cm), a conventional biliary FCSEMS (long stent; 8 or 10 mm in diameter, 6 or 8 cm in length) was used. |
|
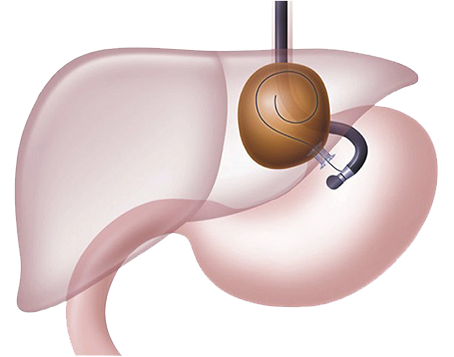 |
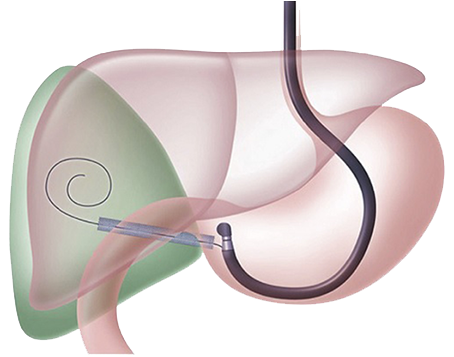
Figure 1. Schema of EUS-guided drainage of HA using a short and large diameter biflanged self-expandable metal stent (short SEMS) |
| The technical success rate was 100% and the clinical success rates of EUS-HAD and EUS-BLD at the first session were 71.4% and 83.3%, respectively. In 2 cases, they needed necrosectomy (endoscopic necrotic tissue removal) as an additional therapy. The final clinical success rate was 100%. There were no procedure-related adverse events and no cases of recurrence during the follow-up period (median, 83.5 days). We think EUS-guided drainage has several advantages over PCD as follows: 1) one-step internal drainage is suitable for patients not only for cosmetic reasons but also for physiologic liquid flow; 2) there is no risk of self-removal of the external drain, which causes peritonitis; 3) possible drainage of the lesion around the caudate lobe where puncture may be difficult. Furthermore, a 10-mm-diameter fully covered or 16-mm-diameter fully covered self-expandable metal stent (SEMS) may have several advantages compared with 1 or more conventional PS for treatment by EUS-HAD and EUSBLD as follows: 1) only 1 stent is required because of the large diameter; thus, FCSEMS placement may allow fewer sessions and reduce the procedure time; 2) minimum leakage of liquid in the cavity; 3) upon FCSEMS placement, sufficient drainage is expected, leading to rapid improvement; 4) DEN can be easily performed through the large-bore stent, as was seen in this study, as DEN was easily performed through the FCSEMS in 2 cases; and 5) FCSEMSs may be helpful for hemostasis when unexpected bleeding from the tract occurs during the procedure. |
|
|
|
Figure 2. Schema of EUS-guided drainage of biloma using a usual long biliary self-expandable metal stent (long SEMS) |
| The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth. |
|